
Our State of the
Art Office
Art Office
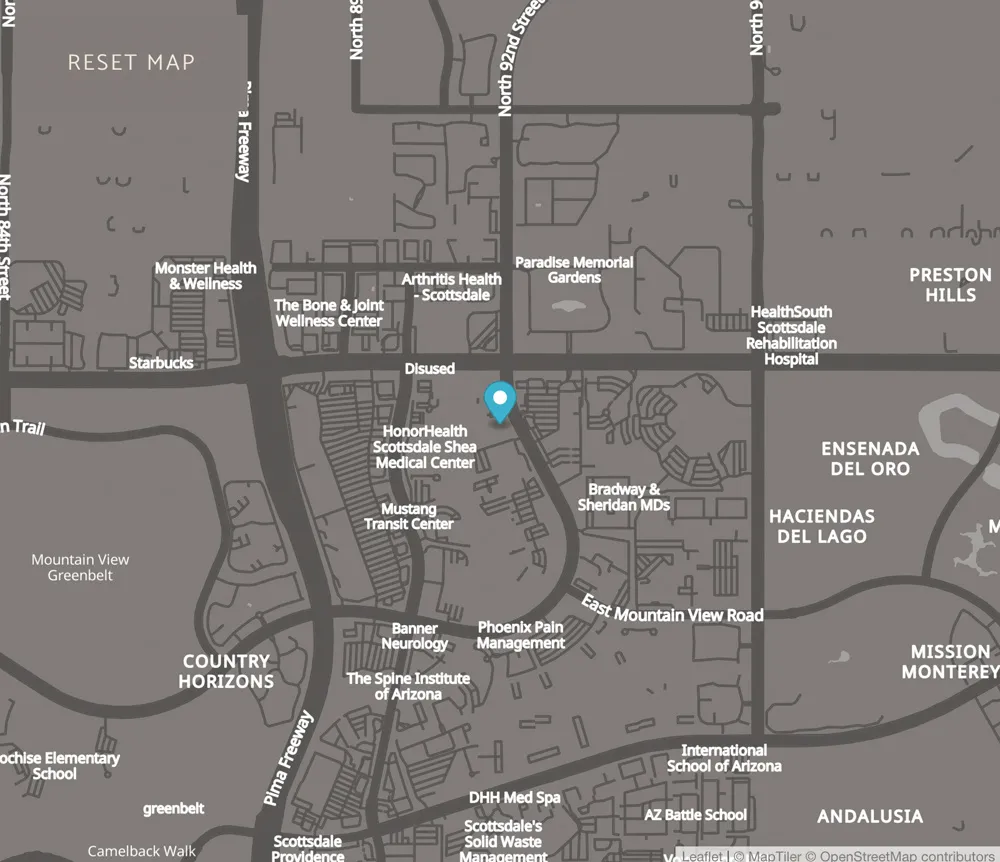
10250 N 92nd St Ste 301
Scottsdale, AZ 85258
Fax: (480) 896-0599
Office Hours
Tuesday:
8:00 AM - 4:00 PM
Wednesday:
8:00 AM - 4:00 PM
Thursday:
8:00 AM - 4:00 PM
Friday:
8:00 AM - 4:00 PM
Office Hours
Tuesday through Friday:
8:00 AM - 4:00 PM
Find Us Online
Have Questions? Contact Us Today!
Serving Across the Entire United States
Serving the Following Regions
- Utah
- Colorado
- New Mexico
- Nevada
- Arizona
Serving the Following Cities
- Phoenix AZ
- Tuscon AZ
- Glendale AZ
- Tempe AZ
- Mesa AZ
- Chandler AZ
- Flagstaff AZ
- Prescott AZ





Dental Website Design by PBHS © 2026